Bedside Topline (What to Remember in a Crisis)
- IABP = counterpulsation: inflates in diastole, deflates just before systole
- Goals: ↑ coronary perfusion, ↓ LV afterload, ↓ myocardial O₂ demand, modest ↑ cardiac output
- Timing: Inflate on the dicrotic notch; deflate halfway down the diastolic downslope before the next systolic upstroke
- Waveform: Augmented diastolic pressure should be the tallest peak; assisted systolic should be slightly lower than unassisted systolic
- Critical: Timing errors hurt — late deflation is the worst (actually ↑ afterload and myocardial work)
Quick Reference
- Primary Use: Temporary mechanical circulatory support for cardiogenic shock, high-risk PCI, and post-cardiotomy support
- Mechanism: Counterpulsation — diastolic inflation increases coronary perfusion, systolic deflation reduces afterload
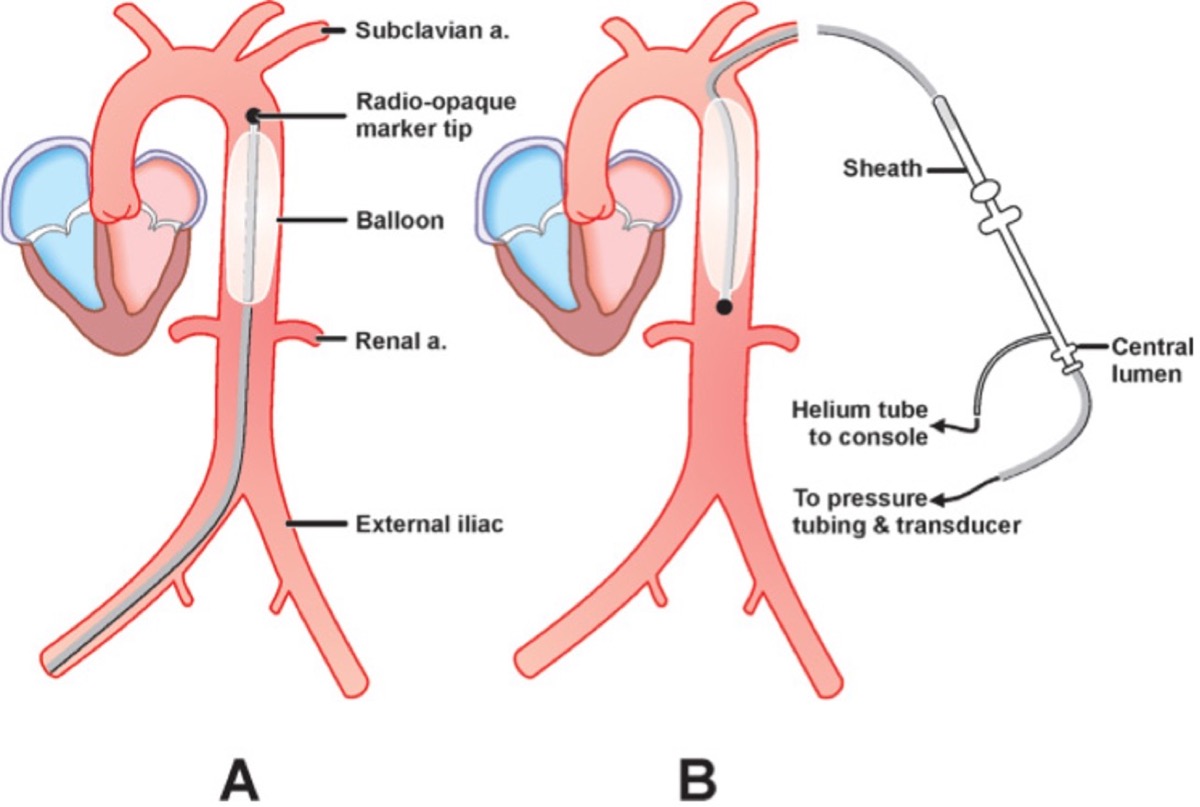
- Position: Proximal descending thoracic aorta, 1-2 cm distal to left subclavian artery
- Gas: Helium (low density for rapid movement, inert, rapidly absorbed if leak)
- Volume: 25-50 mL depending on patient height
- Expected benefit: Modest ↑ stroke volume/cardiac output (0.5-1.0 L/min), improved perfusion pressures
- Key limitation: Requires organized ventricular contraction — minimal benefit in VF/VT or severe LV standstill
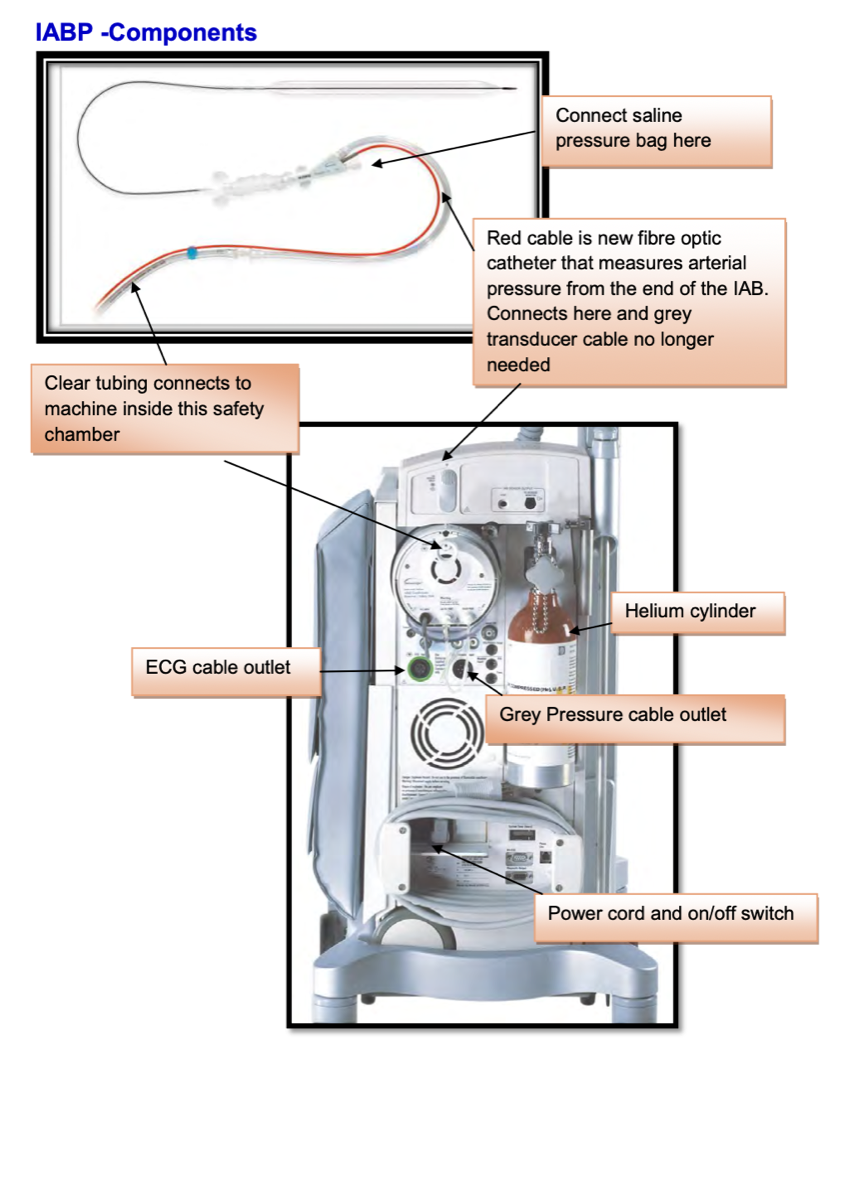
Device Overview
Core Physiology & Hemodynamic Effects
What the Balloon is Doing
- Sits in proximal descending thoracic aorta, 1-2 cm distal to the left subclavian origin
- Volume ~25-50 mL depending on patient height
- Filled with helium (very low density → rapid movement; inert and rapidly absorbed if leak)
- Inflation in early diastole displaces blood both proximally (toward aortic root/coronaries) and distally (toward visceral and peripheral beds)
- Deflation just before systole creates a transient 'vacuum' in the aorta → ↓ aortic end-diastolic pressure → ↓ LV afterload and earlier aortic valve opening
Primary Hemodynamic Effects
- ↑ Diastolic aortic pressure → ↑ coronary perfusion (especially subendocardium)
- ↓ LV afterload → ↓ LV wall tension and ejection pressure
- ↓ Duration of isovolumetric contraction (major O₂-consuming phase) → ↓ myocardial O₂ demand
- Net: modest ↑ stroke volume/cardiac output (often 0.5-1.0 L/min), improved systemic perfusion pressures
Secondary/Systemic Effects (Variable)
- ↓ Pulmonary capillary wedge/LA pressures (offloading LV)
- ↓ SVR (functional afterload reduction)
- ↑ Cerebral and renal perfusion pressures when MAP improves
Benefit depends on: rhythm, native LV function, aortic compliance, balloon volume, and position.
IABP Flow Demonstration
IABP inflation/deflation demonstration showing counterpulsation mechanics
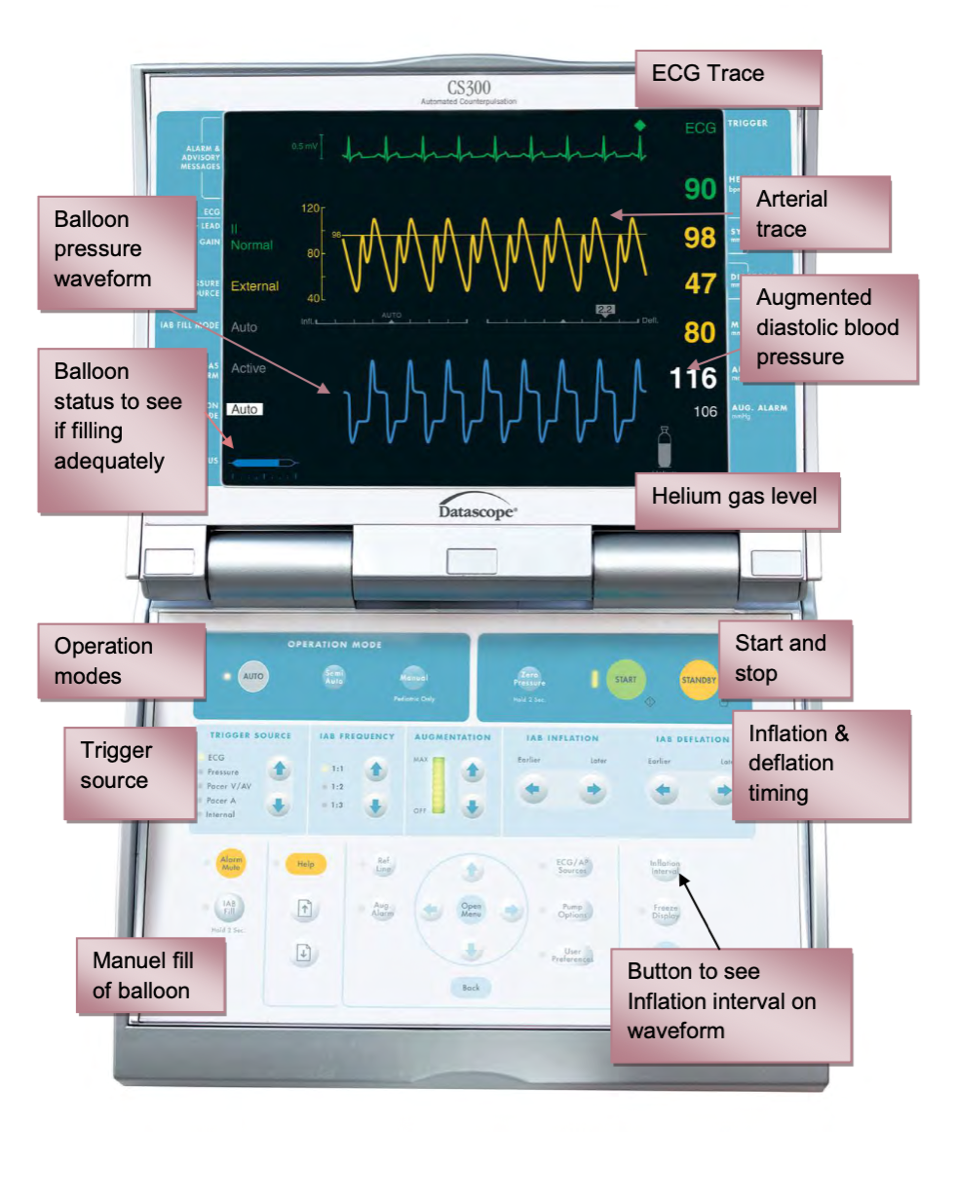
Normal Timing & Waveform Fundamentals
Think in terms of the arterial line – the IABP is just reshaping that waveform.
Key Features of a Normal Assisted Beat
- Unassisted systolic pressure: the native peak on an unassisted beat
- Dicrotic notch: marks aortic valve closure — this is your reference for inflation
- Augmented diastolic peak: tallest peak, appears immediately after the dicrotic notch when balloon inflates
- Assisted end-diastolic pressure: lowest point just before the next systolic upstroke — should be lower than the unassisted end-diastolic pressure
- Assisted systolic pressure: systolic peak after deflation — should be slightly lower than unassisted systolic pressure
Rules of Thumb for Correct Timing
- Inflation: sharp 'V' at the dicrotic notch; augmented diastolic peak immediately after
- Deflation: trough occurs halfway down the diastolic downslope before the next systolic upstroke
- Assisted end-diastolic pressure < unassisted end-diastolic pressure
- Augmented diastolic peak > unassisted systolic peak
Clinical Pearl: Check timing in 1:2 mode so you can compare assisted vs unassisted beats side by side.
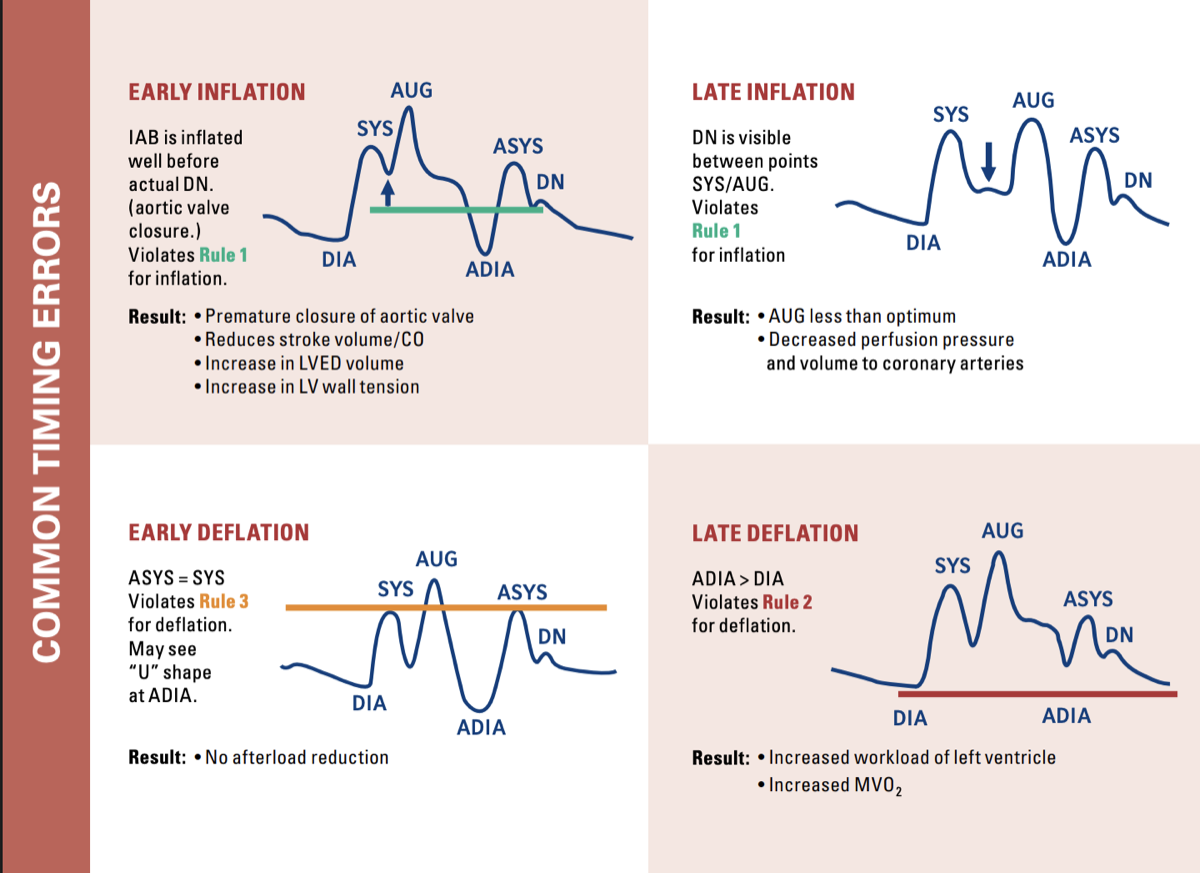
Timing Error Recognition
Classic arterial waveform patterns and what they mean:
Swipe to see more
| Error | Waveform Clues | Physiology | What to Adjust |
|---|---|---|---|
| Early Inflation | Augmented diastolic peak merges into systolic peak; diastolic 'bump' starts before dicrotic notch; no clear V-notch | Balloon inflates while aortic valve still open → premature aortic valve closure, ↑ LVEDV/LVEDP, ↑ afterload, risk of aortic regurg and ↑ MVO₂ | Delay inflation (move trigger later) until just at the dicrotic notch |
| Late Inflation | Inflation well after dicrotic notch; augmented diastolic peak small and delayed; augmented diastolic < unassisted systolic | Missed chance to push blood into coronaries at onset of diastole → suboptimal coronary perfusion, minimal benefit | Advance inflation (move earlier) so balloon inflates exactly at the dicrotic notch |
| Early Deflation | Sharp early drop after augmented diastolic peak; wide U-shaped trough; assisted end-diastolic ≈ or > unassisted end-diastolic; assisted systolic may be higher | Lose afterload reduction; aortic pressure returns to baseline before systole, possible retrograde coronary/carotid flow; ↑ MVO₂ | Delay deflation slightly (move later) so trough is immediately before systolic upstroke, and lower than unassisted diastolic |
| Late Deflation (WORST) | Augmented diastolic peak looks widened; assisted end-diastolic ≈ unassisted; slow, blunted upstroke of assisted systolic | LV begins ejecting against still-inflated balloon → ↑ afterload, prolonged isovolumetric contraction, major ↑ MVO₂; pump can actually impede LV ejection | Advance deflation (earlier) so balloon empties before the aortic valve opens |
Late deflation is the worst timing error — it actually increases afterload and myocardial work, the opposite of what you want!
Triggers, Modes, and Weaning
Trigger Options
- ECG (R-wave): preferred trigger; best when QRS is tall/consistent
- Arterial pressure (AP): useful in atrial fibrillation, paced rhythms, or noisy ECG; uses upstroke of arterial waveform
- Internal/asynchronous: last resort (e.g., during arrest with no reliable ECG/AP); keeps balloon moving to limit thrombus but does not provide true counterpulsation
Assist Ratios
- 1:1 — balloon inflates every beat; default for shock and transport; maximal support
- 1:2 — every second beat assisted; used to check timing and during early weaning
- 1:3 — minimal support; late weaning step in stable patients
Typical Weaning Approach
(Institutional protocols vary)
- Confirm readiness: CI ≥ ~2.2-2.5 L/min/m², MAP ≥ 65 mmHg, no escalating vasoactive support, rhythm stable
- Stepwise reduce assist ratio (1:1 → 1:2 → 1:3) while keeping balloon volume unchanged
- Reassess hemodynamics, lactate, and perfusion with each step; if MAP, CI, or symptoms worsen, step back up
- Only once stable on low assist (e.g., 1:3) do you proceed to removal
Key Point: Never reduce balloon volume during weaning — this increases clot risk. Only reduce frequency (assist ratio).
Indications, Contraindications, and Limitations
Common Real-World Indications
- Cardiogenic shock after acute MI (especially LV failure with ongoing ischemia)
- Mechanical complications of MI — acute severe MR (papillary muscle rupture) or VSD as a bridge to surgery
- Refractory unstable angina/ongoing ischemia despite maximal medical therapy
- Post-cardiotomy low-output syndrome and difficulty weaning from bypass
- Bridge to more definitive support (LVAD/ECMO) or to high-risk PCI/CABG in selected patients
- Refractory ventricular arrhythmias
- Cardiotoxicity (e.g., verapamil overdose)
Key Contraindications (Absolute/Strong Relative)
- Severe aortic regurgitation (balloon inflation worsens regurgitant volume)
- Aortic dissection or significant thoracic/abdominal aortic aneurysm
- Severe peripheral vascular disease or iliac occlusive disease where catheter would critically reduce flow
- Uncontrolled bleeding or severe coagulopathy may make insertion/removal unsafe
- Patent ductus arteriosus
- Thoracic aortic graft <12 months old
Important Limitations to Remember
- Requires organized ventricular contraction — minimal benefit in severe LV standstill or VF/VT without perfusing beats
- Does not directly support RV failure or isolated right-sided cardiogenic shock
- Effect size is modest compared with ECMO/LVAD — think of it as a 'fine-tuning' device rather than a full replacement pump
- Benefit is highly dependent on correct timing and rhythm; AF with RVR or frequent ectopy can reduce effectiveness
- Requires minimum cardiac index of 1.2-1.4 L/min/m² for clinical benefit
- Heart rate >130 bpm reduces efficiency
Remember: IABP use requires potential for spontaneous recovery or planned corrective intervention. It's a bridge, not a destination.
Bedside & Transport Pearls
- Always travel with: a charged pump, spare helium tank, and reliable power source; verify battery status before leaving
- Keep the IABP running whenever possible — a static balloon is a thrombus magnet; if off, manually inflate/deflate per protocol
- Patient positioning: leg with femoral catheter straight; avoid hip flexion; log-roll rather than sit-up if possible
- Monitor distal limb perfusion (pulses, Doppler, color, temperature, cap refill) at least hourly or per unit policy
- Watch urine output and renal function — low output may suggest low flow or balloon too distal (obstructing renal arteries)
- Secure all tubing and cables; avoid tension on the catheter during transfers and log-rolls
- Use gentle sedation/analgesia to control anxiety and prevent leg movement while preserving hemodynamics
- Defibrillation/cardioversion: the pump is isolated/protected, but everyone still needs to be 'clear'
- In cardiac arrest: consider arterial-triggered or internal-trigger modes to keep the balloon moving during CPR if there is an adequate pressure signal
Transport Tip: Have a plan for defibrillation before leaving the unit. Know your battery life and have backup power ready.
Troubleshooting & Red Flags
Alarms & What They Usually Mean
- Loss of trigger: check ECG quality, lead placement, cables; if needed, switch to arterial trigger
- Loss of pressure waveform: check pressure bag, tubing, stopcocks, transducer level/zero, or use an alternate arterial line
- Gas leak / rapid helium loss: inspect catheter/tubing for kinks or disconnections; look for blood in the helium tubing → suspect balloon rupture → stop pump and notify provider immediately
- High plateau pressures: may indicate hypertension, reduced aortic compliance, or incorrect balloon volume/position
- Low plateau pressures: may indicate hypotension, low SVR, or underfilled balloon; correlate with patient and console settings
Clinical Red Flags Requiring Urgent Review
- Sudden loss of augmentation or major change in waveform shape not explained by timing adjustments
- Acute limb ischemia: cool, pale, painful leg or loss of pulses on the catheter side
- New or worsening chest pain, pulmonary edema, or hemodynamic collapse despite the pump
- Hematuria, rising creatinine, or anuria suggesting renal ischemia
- Any suspicion of balloon rupture (blood in helium line, unexplained gas loss)
Complications
During use:
- Limb ischemia (up to 25%)
- Helium embolism from balloon rupture
- Hemolysis
- Thrombocytopenia
- Peripheral neuropathy
- Infection
During/after removal:
- Hematoma
- Pseudoaneurysm
- Arteriovenous fistula
- Catheter entrapment
References
- Khan, T. M., & Siddiqui, A. H. (2022). Intra-aortic balloon pump. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK542233/
- Nekic, P. (2016). Intra-aortic balloon counterpulsation learning package. Liverpool Hospital ICU.
- Yartsev, A. (2015). Intra-aortic balloon pump. Deranged Physiology. https://derangedphysiology.com
- IA MED. (2018). IABP timing guide and waveform exercises. IA MED Education.
- Nickson, C. (2024). Intra-aortic balloon pump. Life in the Fast Lane. https://litfl.com/intra-aortic-balloon-pump/
Medical Disclaimer
- For Educational Purposes Only: This content is intended for educational reference and should not be used for clinical decision-making.
- Not a Substitute for Professional Judgment: Always consult your local protocols, institutional guidelines, and supervising physicians.
- Verify Before Acting: Users are responsible for verifying information through authoritative sources before any clinical application.
AI Assistance Notice
AI was used to assist in organizing and formatting this information. All content is reviewed for accuracy.