Bedside Snapshot
Goal
Establish emergency oxygenation and ventilation through the cricothyroid membrane when all other airway methods fail
Key Indication
Cannot-intubate, cannot-oxygenate (CICO) after failed intubation, BVM, and supraglottic airways
Critical Landmark
Cricothyroid membrane - soft depression between thyroid cartilage (above) and cricoid cartilage (below)
Must Remember
When CICO is recognized, perform cricothyrotomy immediately - hesitation is lethal
What is Cricothyrotomy?
Cricothyrotomy is an emergency surgical airway established through the cricothyroid membrane between the thyroid and cricoid cartilages. It's the definitive rescue airway when all non-surgical options have failed.
Think of it as the "parachute" of airway management: You hope you never need it, but when you do, hesitation or poor preparation is lethal.
Role in Difficult Airway Management
- Final step of the difficult airway algorithm
- Rescue airway, not a primary strategy in most adults
- Must be performed promptly once CICO is recognized
- Preferred over tracheostomy in emergencies - faster, easier access
Pearl: When done decisively and correctly, cricothyrotomy can be life-saving within seconds to minutes. Delays lead directly to hypoxic brain injury and cardiac arrest.
Indications
Primary Indication: Cannot-Intubate, Cannot-Oxygenate (CICO)
- Failed attempts at endotracheal intubation AND
- Inadequate oxygenation/ventilation despite BVM and supraglottic airways
Other Critical Indications
- Severe upper airway obstruction where transoral/nasal intubation is impossible:
- Massive facial trauma, midface fractures
- Oropharyngeal hemorrhage
- Upper airway burns with rapidly progressing edema
- Angioedema or anaphylaxis with near-complete obstruction
- Entrapped/confined patients where access to the face is severely limited
Critical Decision Point: In true CICO, loss of life from hypoxia outweighs most contraindications. If you cannot oxygenate by any other means, cricothyrotomy is indicated.
Relative Contraindications
- Very young children (<8-10 years): cricothyroid space is small - needle cric with transtracheal ventilation preferred
- Laryngeal/tracheal disruption below the cricothyroid membrane
- Significant anatomic distortion at the membrane (tumor, previous surgery) - may require alternative approach
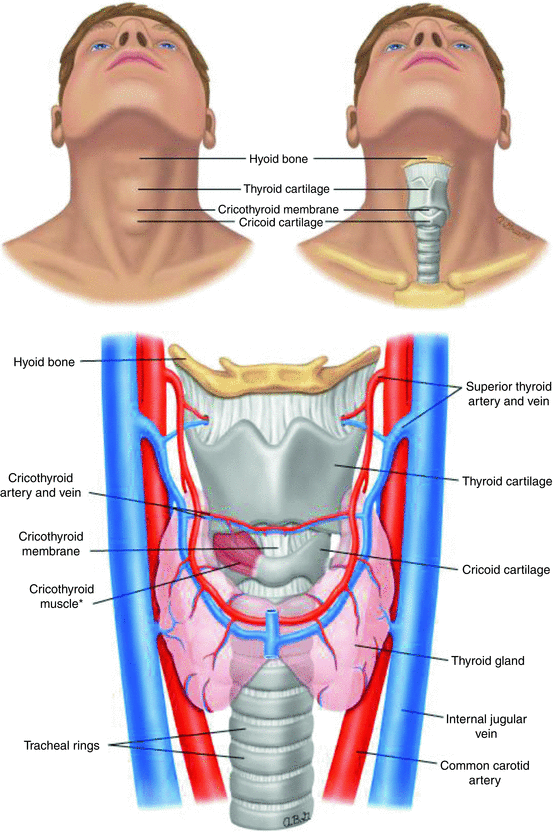
Anatomy & Landmarks
Understanding surface anatomy is critical for safe and rapid cricothyrotomy.
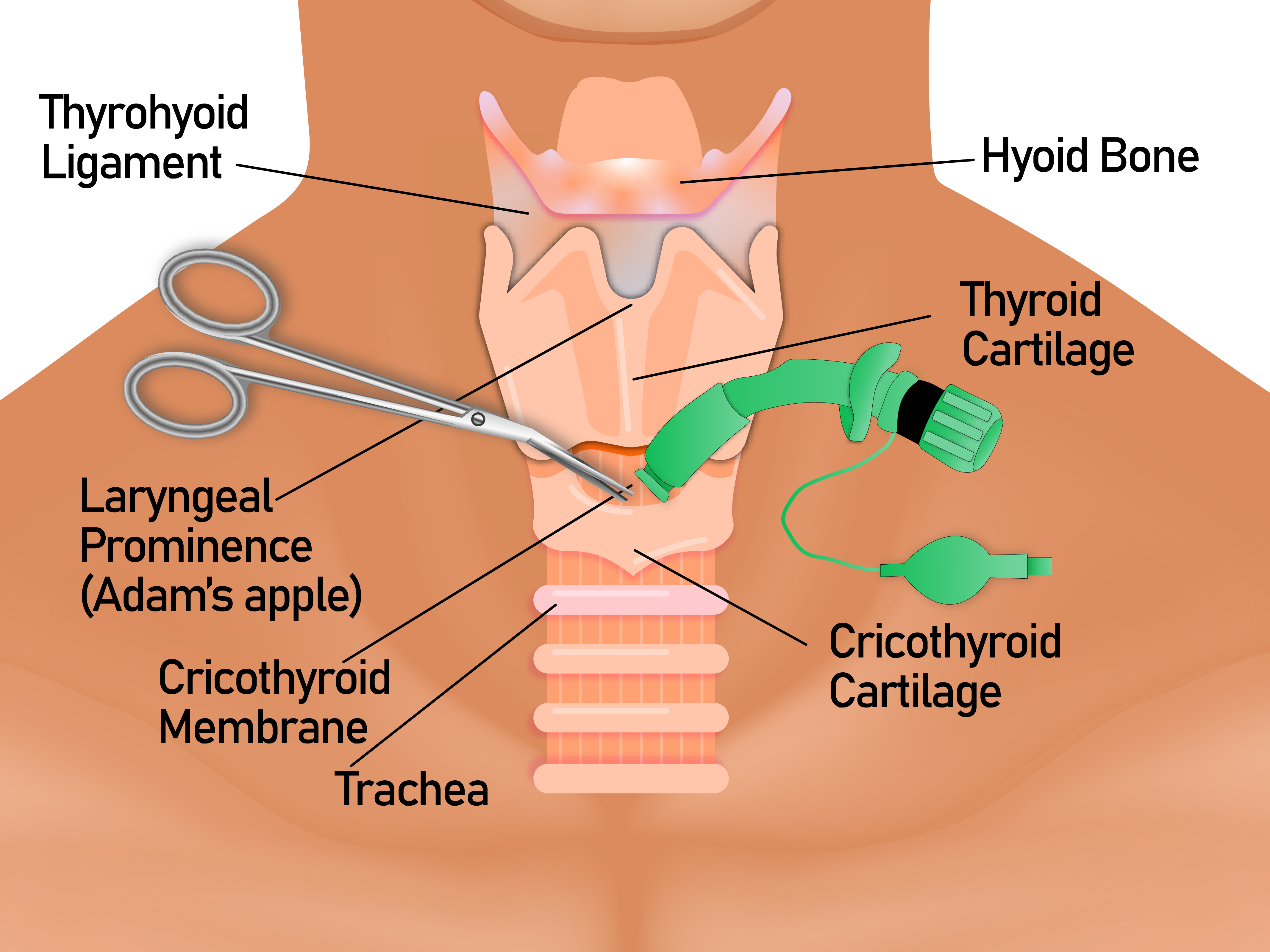
Key Structures
- Thyroid cartilage: Prominent "Adam's apple" - palpate from superior to inferior to find midline prominence
- Cricothyroid membrane: Soft, slightly indented space immediately below thyroid cartilage - this is your TARGET
- Cricoid cartilage: Firm, circumferential ring below the membrane - serves as inferior landmark
Landmarking Technique: "Laryngeal Handshake"
- Stabilize the larynx with one hand
- Identify the thyroid cartilage prominence
- Walk your fingers downward
- Feel for the soft depression (cricothyroid membrane)
- Confirm the firm cricoid ring below
Pearl: In obese or edematous patients, apply firm progressive pressure through soft tissues until you feel the firm cartilage. In trauma with distorted anatomy, use a vertical midline incision and careful blunt dissection to find the membrane.
Equipment
Have a dedicated cricothyrotomy kit or standardized "scalpel–bougie–tube" setup ready wherever advanced airway management occurs.
Surgical Cricothyrotomy Setup (Adult)
- PPE: Gloves, eye protection, mask
- Antiseptic: Chlorhexidine or povidone-iodine (if time allows)
- Scalpel: #10 or #11 blade
- Tracheal hook or hemostat (for dilation and control)
- Bougie (gum elastic bougie) or appropriate introducer
- Cuffed ETT: 6.0 mm for most adults
- Syringe for cuff inflation
- Suction (Yankauer)
- Securing device: Tape or commercial tube holder
Needle Cricothyrotomy Setup (Pediatrics)
- Large-bore catheter: 14-gauge for adults, 16-18-gauge for children
- Syringe with saline for aspiration confirmation
- Oxygen source with jet insufflation system or modified BVM connection
- Capnography if available
- Backup plan for surgical conversion
Note: Know what your service stocks and practice with that specific equipment in simulation. Several commercial pre-packaged kits exist with pre-sized tubes, dilators, and introducers.
Technique: Scalpel-Bougie-Tube Method
The scalpel-bougie-tube technique is widely taught and uses commonly available equipment.
Time is Critical: This procedure should be rapid and focused. Minutes or seconds matter in CICO scenarios.
Preparation
- Call for help and declare "cannot-intubate, cannot-oxygenate" emergency
- Position: Supine with neck extended (use shoulder roll); maintain C-spine precautions if trauma
- Antiseptic: Apply if time allows, but DO NOT delay procedure
- Continue oxygenation attempts with BVM/SGA while preparing
Step-by-Step Procedure
Step 1: Landmark and Stabilize
- Palpate thyroid cartilage, then cricothyroid membrane in midline
- Stabilize larynx with non-dominant hand
- DO NOT let go of landmarks
Step 2: Vertical Skin Incision
- Make 3-4 cm vertical midline skin incision over cricothyroid membrane
- Vertical incision is more forgiving - helps you find membrane even if landmarks are imperfect
Step 3: Identify the Membrane
- Bluntly dissect through subcutaneous tissue with finger or hemostat
- Feel for firm thyroid and cricoid cartilages
- Palpate the soft space between them
Step 4: Horizontal Membrane Incision
- Make horizontal stab incision through cricothyroid membrane with scalpel
- Turn blade 90° so sharp edge faces inferiorly (toward feet)
- Gently dilate the incision
Pearl: Vertical skin incision, horizontal membrane incision. This is the key to safe cricothyrotomy.
Step 5: Insert Bougie
- Keep scalpel in place or use finger/hemostat to maintain opening
- Slide bougie through incision into trachea, aiming caudally
- You may feel tracheal rings or "clicks" as confirmation
Step 6: Railroad the Tube
- Thread 6.0 mm cuffed ETT over bougie into trachea
- Advance until cuff is just past membrane (only 3-4 cm beyond skin)
- Avoid inserting too deeply
Step 7: Confirm and Inflate
- Remove bougie
- Inflate cuff with air
- Attach BVM or ventilator
- Confirm with waveform capnography, chest rise, and auscultation
Step 8: Secure and Manage
- Control bleeding with direct pressure around (not on) the tube
- Secure tube with tape or commercial holder
- Reassess frequently for kinking or displacement
Needle Cricothyrotomy (Temporizing)
Needle cricothyrotomy is primarily a temporizing measure, more commonly used in smaller children. It provides oxygenation but not effective CO₂ elimination.
Key Concept: Needle cric buys time for a definitive airway - it is NOT a long-term solution.
Technique
- Landmark: Identify and stabilize cricothyroid membrane
- Insert needle: Use 14-gauge catheter at 45° angle caudally while aspirating with saline-filled syringe
- Confirm: Stop when you see air bubbles (tracheal placement)
- Advance catheter: Slide catheter into trachea while withdrawing needle
- Connect oxygen: Use jet ventilation system or modified BVM with high-flow O₂
- Ventilate: 1 second insufflation, 3-4 seconds passive exhalation
Complications to Monitor: Barotrauma, subcutaneous emphysema, inadequate CO₂ clearance. Plan for rapid conversion to surgical airway.
Complications & Troubleshooting
Misplacement or False Passage
- Signs: No capnography, poor chest rise, subcutaneous emphysema
- Management: Stop, reassess anatomy, repeat procedure if patient remains in CICO
Hemorrhage
- Cause: Bleeding from skin vessels or thyroid isthmus
- Management: Apply direct pressure around (not on) the airway; suction as needed; proceed decisively
Subcutaneous Emphysema and Barotrauma
- More common with: Needle cric and jet ventilation, insufficient exhalation
- Prevention: Monitor chest rise, allow adequate exhalation times
Esophageal or Posterior Wall Injury
- Prevention: Avoid aggressive downward angulation; aim strictly midline and just through membrane
Tube Obstruction or Kinking
- Cause: Small-diameter tubes, sharp neck flexion
- Prevention: Use 6.0 ETT, check for kinks, maintain neutral neck position
Long-term Management: Cricothyrotomy is usually temporary. ENT or surgery should convert to formal tracheostomy in a controlled setting as indicated.
Pearls & Training
Clinical Pearls
- Vertical skin, horizontal membrane: This combination is safest and most effective
- Stabilize and don't let go: Keep your non-dominant hand on landmarks throughout
- Declare CICO early: Don't wait until cardiac arrest - perform cric when indicated
- 6.0 ETT is ideal: Balance between adequate lumen and ease of insertion
- Shallow insertion: Only 3-4 cm beyond skin - too deep risks right mainstem or carina injury
Training Tips
- Practice on task trainers and cadaver labs - muscle memory is critical
- Train entire team on difficult airway algorithm and CICO recognition
- Rehearse scalpel-bougie-tube sequence regularly ("mental reps")
- Ensure cric kits are standardized, complete, and checked routinely
- Use simulation scenarios where cricothyrotomy is the only correct solution
- Debrief after cases: Was CICO recognized early enough?
Final Pearl: Cricothyrotomy is a skill that must be performed with confidence and speed. Regular training and simulation are essential because you won't have time to think during a real CICO event.
Medical Disclaimer
- For Educational Purposes Only: This content is intended for educational reference and should not be used for clinical decision-making.
- Not a Substitute for Professional Judgment: Always consult your local protocols, institutional guidelines, and supervising physicians.
- Verify Before Acting: Users are responsible for verifying information through authoritative sources before any clinical application.
AI Assistance Notice
AI was used to assist in organizing and formatting this information. All content is reviewed for accuracy.