- Acidosis (pH <7.1)
- Electrolytes (K+ ≥6.0 + ECG Δ)
- Intoxications (dialyzable)
- Overload (pulmonary edema)
- Uremia (pericarditis, encephalopathy)
- AV Fistula (preferred)
- AV Graft
- Tunneled catheter
What is Hemodialysis?
Hemodialysis (HD) is a form of renal replacement therapy (RRT) that uses an extracorporeal circuit and a semipermeable membrane (dialyzer) to remove toxins, correct electrolytes and acid-base disturbances, and remove excess fluid from the blood.
In HD, blood is pumped from the patient through a dialyzer where solute exchange occurs between blood and dialysate (a carefully composed fluid) via diffusion and convection. The "cleaned" blood is then returned to the patient.
HD is used both chronically (end-stage kidney disease, ESKD) and acutely (acute kidney injury, AKI) in hospital settings. In ED/ICU/transport environments, you most often encounter patients who are either:
- ESKD patients coming in with complications from missed or incomplete dialysis, or
- Critically ill patients receiving intermittent HD or continuous RRT as part of multi-organ support
Indications and Goals of Hemodialysis
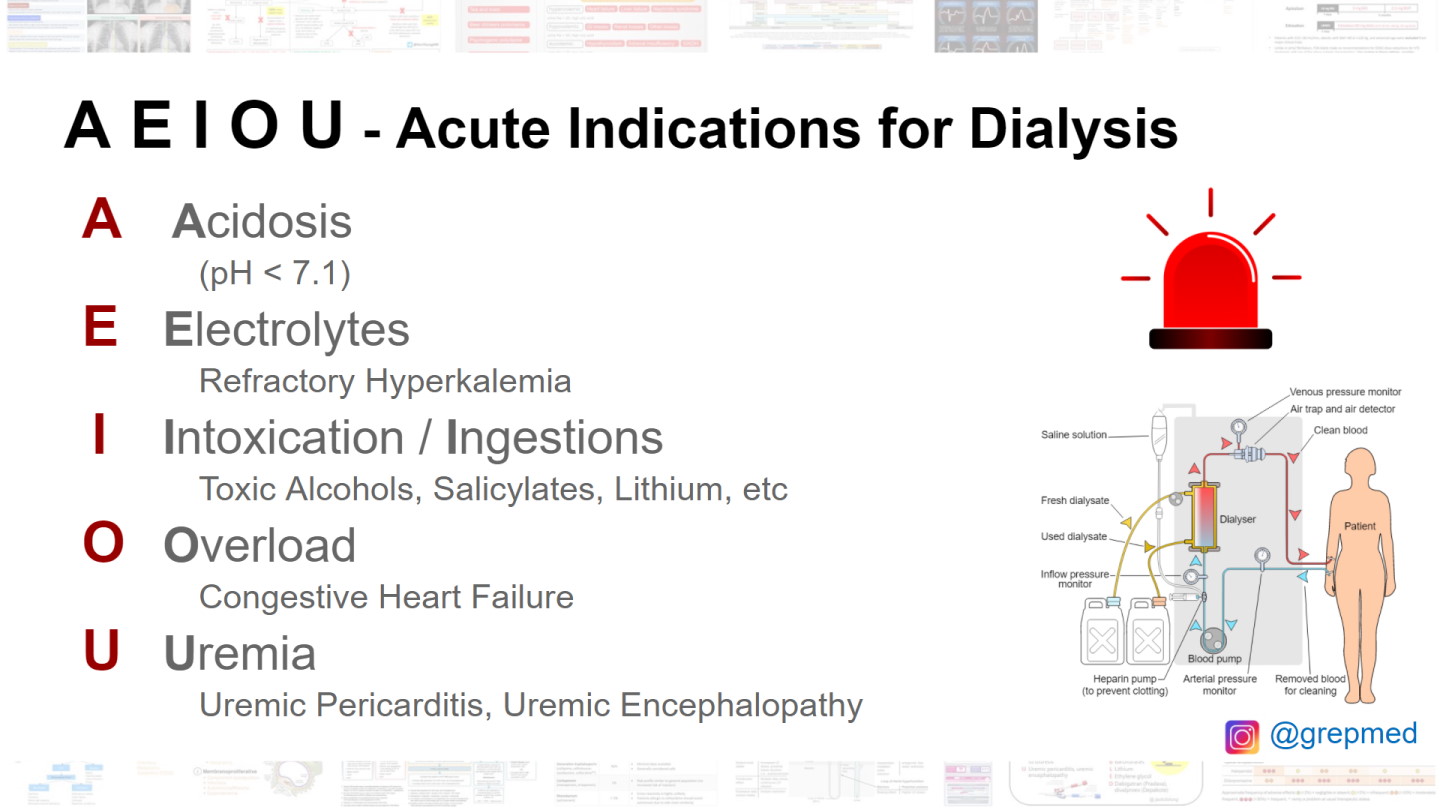
Classic emergent indications are often remembered with the mnemonic "AEIOU":
AEIOU Mnemonic - Urgent Dialysis Indications
- A – Acidosis: Severe metabolic acidosis (often pH < 7.1) not responding to medical therapy
- E – Electrolyte abnormalities: Life-threatening hyperkalemia (e.g., K ≥ 6.0 mmol/L with ECG changes) or other severe electrolyte derangements
- I – Intoxications: Dialyzable toxins (e.g., lithium, salicylates, methanol, ethylene glycol, some drugs depending on protein binding and volume of distribution)
- O – Overload: Refractory volume overload causing pulmonary edema or severe hypertension despite diuretics and medical management
- U – Uremia: Uremic symptoms or complications such as pericarditis, encephalopathy, bleeding diathesis, intractable nausea/vomiting
Broader Goals in Chronic ESKD and ICU Care
- Control volume status: Achieve near-euvolemia (target dry weight) to reduce pulmonary edema, hypertension, and heart failure exacerbations
- Correct electrolytes and acid-base status: Especially potassium, bicarbonate, calcium, and phosphate
- Remove uremic toxins: Improve symptoms such as fatigue, confusion, pruritus, nausea, and reduce long-term complications
- Provide a bridge: Stabilize AKI/ESKD patients while underlying reversible processes are treated or while awaiting renal recovery or transplant
Vascular Access for Hemodialysis
Types of HD Access
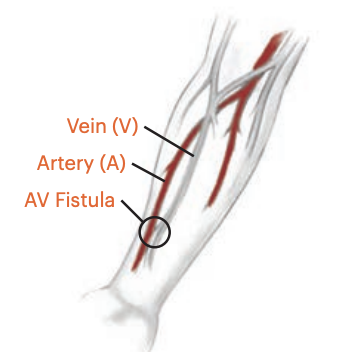
Arteriovenous (AV) Fistula
- Surgical connection between an artery and a vein (e.g., radiocephalic in the forearm)
- Preferred long-term access: Lowest infection and thrombosis risk, best flow and longevity
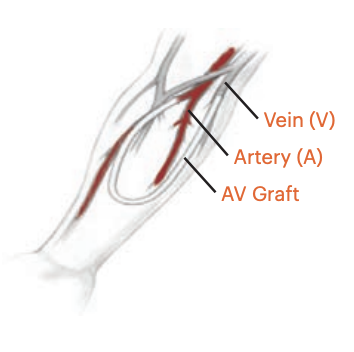
Arteriovenous (AV) Graft
- Synthetic conduit between artery and vein
- Used when native veins are unsuitable; higher infection and thrombosis risk than fistulas
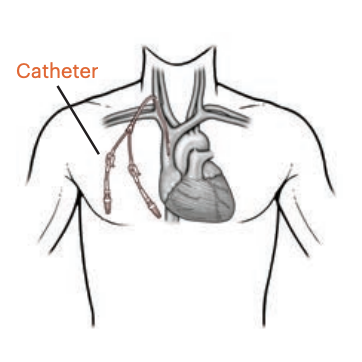
Tunneled Cuffed Dialysis Catheter
- Central venous catheter (commonly internal jugular) with subcutaneous tunnel and cuff
- Used as long-term temporary access or while waiting for AV access maturation; infection risk and central venous stenosis are major issues
Non-tunneled Dialysis Catheter
- Temporary, non-tunneled central line (e.g., IJ, femoral) for urgent or short-term HD in hospital/ICU settings
- Never place IVs, draw blood, or take blood pressures on an arm with a functioning AV fistula or graft unless explicitly cleared by nephrology/vascular surgery
- Protect dialysis catheters: Use only for dialysis unless specifically ordered otherwise; strict aseptic technique and caps in place
- Check fistula/graft patency: Feel for a "thrill" and listen for a "bruit" to confirm flow
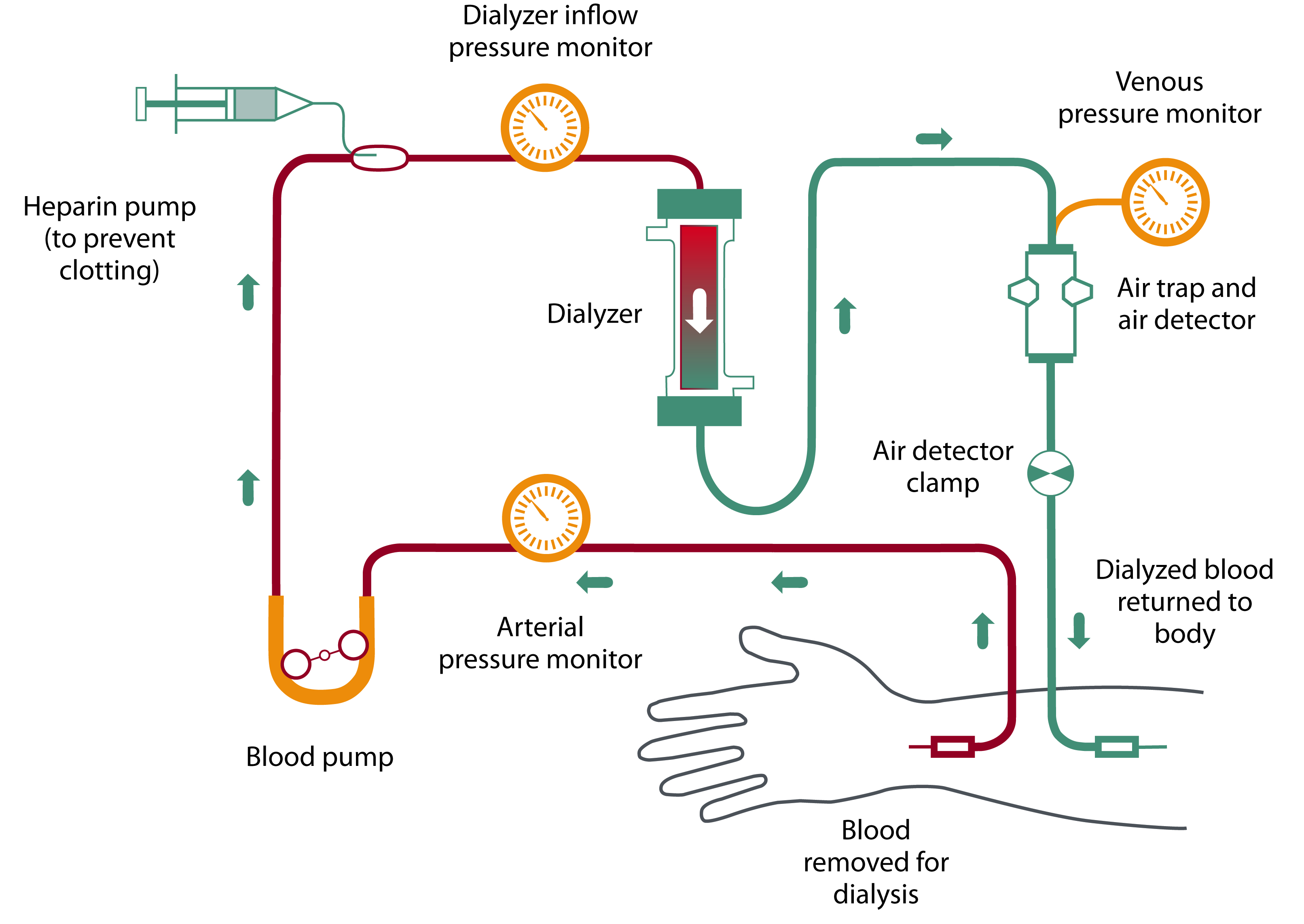
Basic Hemodialysis Circuit and Principles
Core Components of the HD Circuit
- Vascular access: Provides high blood flow (typically 300–500 mL/min in chronic HD)
- Blood pump and lines: Move blood from patient to dialyzer and back
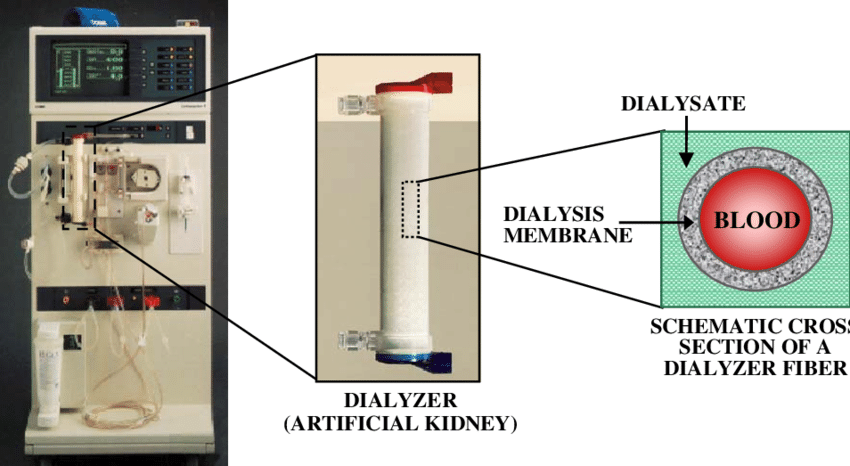
- Dialyzer ("artificial kidney"): Semipermeable membrane where blood and dialysate flow on opposite sides
- Dialysate: Specially formulated solution with controlled concentrations of electrolytes and bicarbonate
- Ultrafiltration control: Regulates how much fluid is removed over time (UF rate)
Physiologic Principles
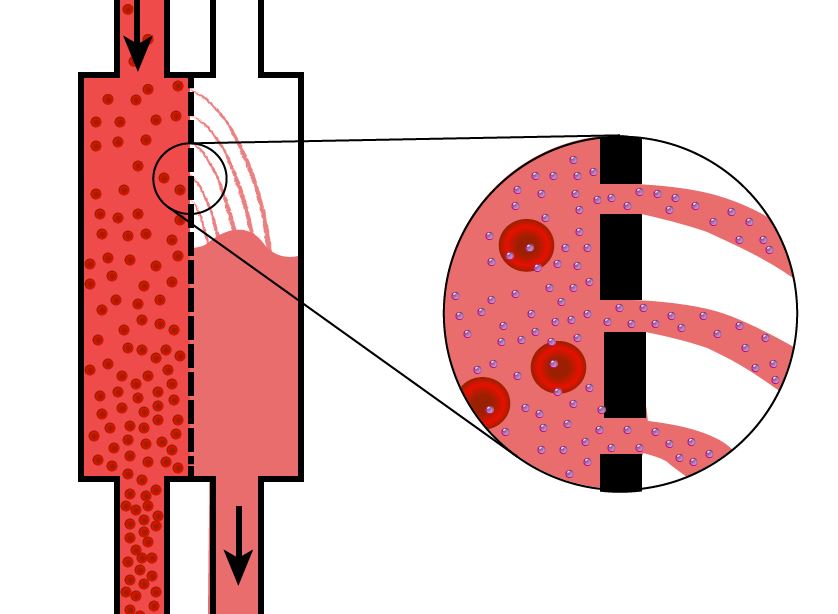
- Diffusion: Solutes move down their concentration gradient across the semipermeable membrane (e.g., urea, potassium, creatinine). Dialysate composition is chosen to pull off excess solutes while maintaining safe levels.
- Convection (ultrafiltration): Fluid removal by creating a pressure gradient across the membrane; solvent drag can remove larger molecules as water is pulled out.
- Volume removal (UF goal): Typically based on pre- and post-dialysis weight difference and assessment of volume status; overly aggressive UF can cause hypotension and ischemia.
- Clearance: Effectiveness depends on blood flow rate, dialysate flow rate, membrane surface area, and session duration.
Typical Hemodialysis Prescription (Big Picture)
A nephrologist writes the detailed HD prescription, but bedside providers should recognize the major components:
Frequency and Duration
E.g., chronic HD 3 times per week, 3–5 hours per session; more frequent/shorter or extended sessions in ICU depending on tolerability.
Blood Flow Rate (Qb)
Often 300–500 mL/min on chronic HD; may be lower in ICU or with limited access.
Dialysate Flow Rate (Qd)
Commonly ~500–800 mL/min; higher flows increase clearance.
Dialysate Composition
- Potassium (K bath): Lower baths (e.g., 1–2 mEq/L) for severe hyperkalemia; higher baths (3–4 mEq/L) to avoid hypokalemia in chronic treatment
- Bicarbonate: Typically 32–38 mEq/L to correct acidosis without overshooting into alkalosis
- Calcium, magnesium, sodium: Adjusted based on labs, bone disease, hemodynamics, and comfort
Ultrafiltration (UF) Goal and Rate
- UF goal: Planned fluid removal (e.g., 2–3 liters) based on pre- vs. target (dry) weight and volume exam
- UF rate: Volume per hour; high UF rates (e.g., >10–13 mL/kg/h) increase risk of intradialytic hypotension and end-organ hypoperfusion
Anticoagulation
Often systemic unfractionated heparin bolus plus smaller maintenance doses; alternatives include regional citrate or heparin-free dialysis in patients with active bleeding or high risk.
Intermittent HD in the ICU vs Chronic Outpatient HD
Chronic Outpatient HD
- Patients typically follow a stable schedule (e.g., Monday-Wednesday-Friday)
- Prescriptions aimed at long-term control of electrolytes, volume status, and uremic symptoms
- Patients are usually more hemodynamically stable and can tolerate higher UF rates and shorter treatments
Intermittent HD in ICU
- Used for AKI or ESKD with critical illness when CRRT (continuous RRT) is unavailable or not required
- Sessions are adjusted for hemodynamic instability: longer duration with lower UF rates can be better tolerated
- Close coordination with ICU staff for vasopressors, ventilator settings, and timing around procedures
- May alternate with or transition to CRRT in severely unstable patients (e.g., high-dose vasopressors, severe ARDS)
Pre- and Post-Dialysis Assessment
Pre-Dialysis Assessment
- Vitals: Blood pressure, heart rate, respiratory rate, SpO₂, temperature
- Weight: Compare to prior weight and target dry weight; estimate fluid overload
- Volume status: Lung sounds, JVD, peripheral edema, work of breathing, orthopnea
- Access check: Inspect fistula/graft/catheter for redness, swelling, bleeding, infection signs; palpate thrill and auscultate bruit
- Symptoms: Dyspnea, chest pain, confusion, nausea/vomiting, pruritus, muscle cramps
- Labs when available: Potassium, bicarbonate, BUN/creatinine, calcium, phosphate, hemoglobin
- Medications: Review timing of antihypertensives, anticoagulants, and other meds that may affect intra-dialytic BP or bleeding
Post-Dialysis Assessment
- Vitals and weight: Assess for hypotension, tachycardia, or overshoot of volume removal
- Symptoms: Resolution or improvement of dyspnea, edema, hyperkalemic ECG changes, uremic symptoms
- Access: Inspect the site (e.g., fistula needle sites for bleeding or hematoma; catheter site for bleeding or infection)
- Mental status: Monitor for dialysis disequilibrium syndrome (headache, nausea, confusion, seizures) especially in first treatments or very high pre-HD urea
- Documentation: UF volume achieved, duration of treatment, any complications or interruptions
Common Complications of Hemodialysis
Intradialytic Hypotension
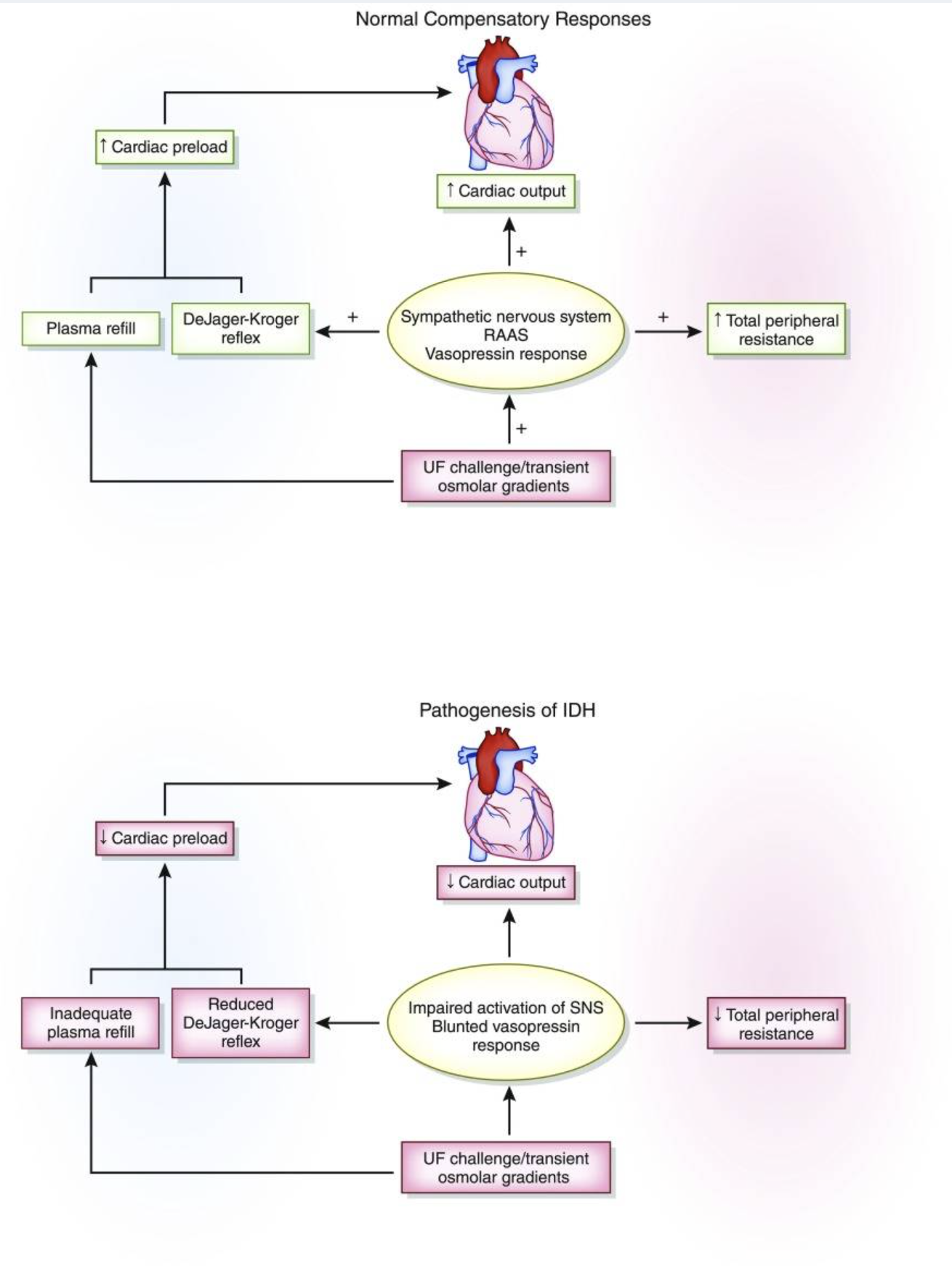
- Very common; often due to rapid UF, autonomic dysfunction, or impaired cardiac function
- Presentation: Dizziness, nausea, cramping, hypotension, syncope
- Management: Decrease UF rate, give small fluid bolus (normal saline), adjust dialysate sodium or temperature per nephrology orders, hold BP meds before HD when appropriate
Muscle Cramps
- Often related to volume removal and shifts in electrolytes
- Treat with UF reduction, stretching, small fluid bolus if appropriate, and reassessing dry weight
Arrhythmias
- Rapid electrolyte shifts (especially potassium and calcium) and volume changes can provoke arrhythmias, including atrial fibrillation and ventricular dysrhythmias
- Monitor continuous ECG in high-risk patients; treat underlying triggers (hyper/hypokalemia, ischemia, hypotension)
Dialysis Disequilibrium Syndrome
- Typically in new HD starts or very high pre-HD BUN when solutes are removed quickly
- Symptoms: Headache, nausea, vomiting, restlessness, confusion, seizures, coma
- Prevention: Slower/shorter initial treatments, gentler clearance; treat supportively and rule out other causes (stroke, hemorrhage, infection)
Access-Related Complications
- Bleeding (from needle sites, graft, or catheter)
- Infection (cellulitis, bacteremia, sepsis from catheters or grafts)
- Thrombosis or stenosis of fistula/graft/catheter leading to poor flows or loss of access
Air Embolism
- Rare but critical; may occur with circuit leaks or line disconnections
- Presentation: Sudden dyspnea, chest pain, hypotension, arrhythmias
- Management: Clamp lines, place patient left lateral decubitus with head down (Durant maneuver) if possible, 100% O₂, call for expert help and hyperbaric consult if available
Allergic/Anaphylactoid Reactions
- Reactions to dialyzer membranes, sterilants, or medications given during HD
- Symptoms: Itching, flushing, dyspnea, hypotension, wheezing, anaphylaxis
- Stop dialysis, treat per anaphylaxis protocols (epinephrine, antihistamines, steroids, airway support)
Electrolytes, Acid-Base, and "Missed Dialysis" Patients
Hyperkalemia
- Common in ESKD patients who miss one or more sessions or with increased tissue breakdown (infection, trauma)
- ED/ICU management: ECG monitoring, IV calcium for membrane stabilization when indicated, insulin + dextrose, beta-agonists, bicarbonate if appropriate, potassium binders, and urgent HD when needed
Metabolic Acidosis
- HD corrects acidosis via bicarbonate in dialysate; severe acidosis is an indication for urgent dialysis when refractory to medical management
Volume Overload and Pulmonary Edema
- Presents with dyspnea, orthopnea, crackles, hypoxemia, hypertension
- May require noninvasive ventilation, vasodilators (e.g., nitrates), and urgent dialysis with careful UF to avoid hemodynamic collapse
- Dyspnea, hyperkalemia, generalized edema, hypertensive crisis, uremic symptoms
- Key steps: Assess ABCs, get ECG and basic labs (K, BUN/Cr, bicarbonate), treat life threats (especially hyperkalemia and pulmonary edema), contact nephrology and the dialysis unit early for urgent HD
- Always ask: "When was your last dialysis session?" and "What is your usual schedule?"
Anticoagulation and Bleeding Risk in HD
Why Anticoagulation is Used
- Heparin is the most common anticoagulant used to prevent clotting in the HD circuit (bloodlines, dialyzer)
- Without anticoagulation, blood clots can form in the circuit, causing treatment interruption and blood loss
Anticoagulation Options
- Standard heparin: Most common; bolus at start, infusion during session; reversible with protamine if needed
- Low molecular weight heparin (LMWH): Less commonly used in HD; different monitoring requirements
- Citrate anticoagulation: Regional citrate anticoagulation (especially in ICU CRRT or for those at high bleeding risk); citrate chelates calcium and is reversed by calcium infusion
- Heparin-free or saline flush: Used in patients at high bleeding risk (post-op, active bleeding, coagulopathy); more frequent circuit clotting possible
Bleeding Risk Considerations
- Uremic patients have platelet dysfunction even before anticoagulation is added
- HD patients on heparin are at increased bleeding risk during and immediately after treatment
- Post-HD bleeding (especially from access sites) can be significant; apply pressure as needed, hold prolonged pressure if on heparin
- Consider heparin-free runs for patients with recent surgery, trauma, GI bleed, intracranial hemorrhage, or coagulopathy
EMS, Transport, and ED Considerations
Common EMS Presentations in HD Patients
- Shortness of breath / pulmonary edema (especially if missed HD or fluid overload)
- Altered mental status (uremia, hyperkalemia, hypotension, stroke, sepsis)
- Hypotension (during or after HD, sepsis, cardiac event)
- Chest pain (CAD is common in this population)
- Bleeding (access site, GI, other sources)
- Syncope or near-syncope (often post-dialysis from volume shifts)
Key EMS/Prehospital Actions
- ABCs; oxygen, IV (but NOT in fistula/graft arm!), cardiac monitor
- Get 12-lead ECG; look for signs of hyperkalemia (peaked T waves, wide QRS, sine wave pattern)
- If hyperkalemia suspected, treat per protocol (calcium, albuterol, etc.)
- Get dialysis history: last session, usual schedule, any recent missed runs
- Know the patient's access type and location—do not use for IV or BP cuff
- NEVER use the fistula or graft arm for IV access or blood pressure
- Do not draw blood from the access arm
- Avoid tight clothing, watches, or restraints on the access arm
ED Priorities for HD Patients
- Stabilize and assess for life-threatening problems: hyperkalemia, pulmonary edema, sepsis, stroke, MI
- Get labs: BMP, CBC, lactate, possibly blood cultures if infection suspected
- Contact nephrology and dialysis center early for urgent or emergent HD if needed
- Document dialysis schedule, last run, and access type in the chart
Dialysis Access Emergencies
- Bleeding from access: Apply direct pressure; elevate; if severe, may need surgical consultation
- Clotted access: No thrill or bruit; refer urgently for declot procedure or new access
- Infected access: Blood cultures, antibiotics, possible removal (especially for catheter infections)
Education and Teaching Tips
For Healthcare Providers
- Always document dialysis schedule and last session in the chart
- Know the patient's access type and protect it from injury, IV placement, and BP cuffs
- Hyperkalemia and pulmonary edema are the most common life-threatening presentations in missed dialysis patients
- Communicate with nephrology early for any unstable HD patient or suspected urgent dialysis need
- Be aware of post-dialysis hypotension and the need for careful fluid management
For Patients and Families
- Attend all scheduled dialysis sessions; missed sessions lead to dangerous fluid and electrolyte buildup
- Follow fluid and diet restrictions (especially potassium and phosphorus)
- Protect your fistula or graft: no blood draws, BP cuffs, or tight clothing on that arm
- Report any signs of infection (redness, swelling, drainage, fever) or access problems (loss of thrill/bruit)
- Know the signs of fluid overload (swelling, shortness of breath, weight gain) and when to seek care
- Keep a list of your medications, dialysis schedule, and nephrologist contact information with you
References
- KDOQI Clinical Practice Guidelines for Hemodialysis Adequacy, 2015 Update.
- Daugirdas JT, Blake PG, Ing TS. Handbook of Dialysis. 5th ed. Wolters Kluwer; 2015.
- George C, Menon A, Gnanamoorthy M. Dialysis Disequilibrium Syndrome: Etiology, Pathophysiology, and Prevention. Am J Med Case Rep. 2018;6(5):89-92.
- National Kidney Foundation. Hemodialysis.
- UpToDate: Technical aspects of hemodialysis initiation; Complications of hemodialysis; Vascular access for hemodialysis.
- American Nephrology Nurses Association. Hemodialysis core curriculum.
Medical Disclaimer
- For Educational Purposes Only: This content is intended for educational reference and should not be used for clinical decision-making.
- Not a Substitute for Professional Judgment: Always consult your local protocols, institutional guidelines, and supervising physicians.
- Verify Before Acting: Users are responsible for verifying information through authoritative sources before any clinical application.