- CAPD: Manual exchanges (4-5/day)
- APD: Automated overnight cycler
- Home-based, patient independence
- Gentler fluid removal
- Preserves residual kidney function
- Peritonitis (cloudy effluent, abdominal pain)
- Exit-site/tunnel infection
What is Peritoneal Dialysis?
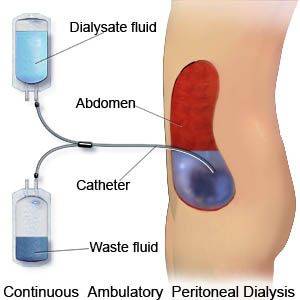
Peritoneal dialysis (PD) is a form of renal replacement therapy that uses the patient's own peritoneal membrane as the semipermeable "dialyzer" to remove waste products, correct electrolytes and acid-base disturbances, and remove excess fluid.
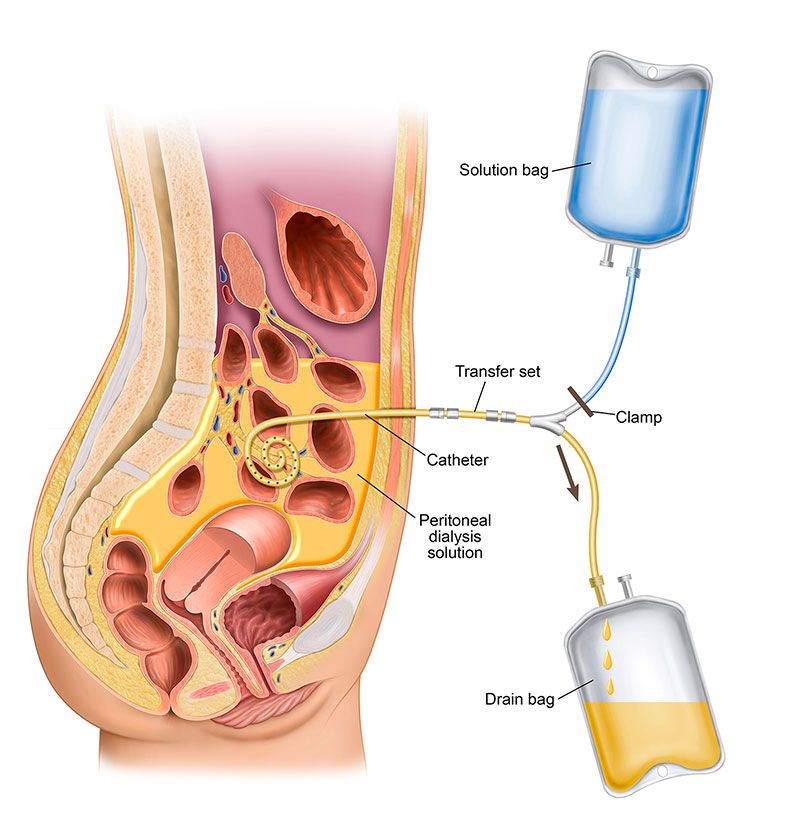
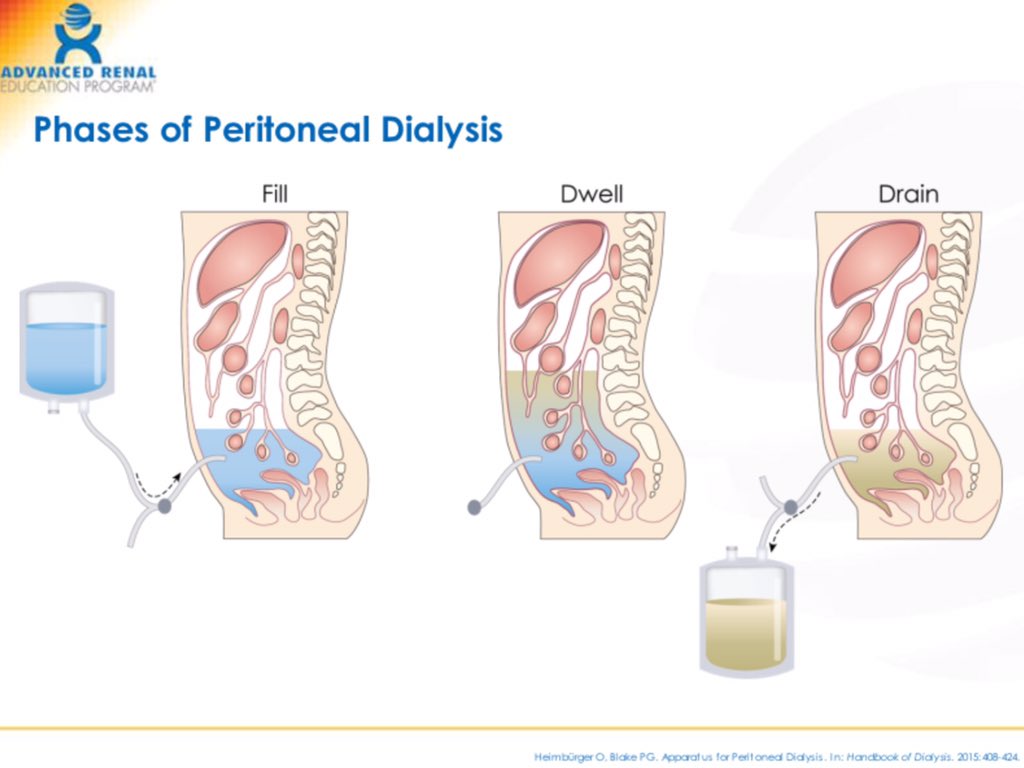
A soft catheter is placed into the peritoneal cavity. Sterile dialysis solution (dialysate) is infused into the abdomen, where it dwells in contact with the peritoneal capillary bed. Solutes and water move between blood and dialysate, and then the used fluid is drained out and replaced with fresh solution.
PD is most commonly a home-based therapy for patients with end-stage kidney disease (ESKD). It can be performed manually during the day (CAPD) or automatically at night using a cycler (APD). Nurses in acute and chronic settings support patient training, monitoring, troubleshooting, and infection prevention.
Types of Peritoneal Dialysis
There are two main types of peritoneal dialysis used in practice:
Continuous Ambulatory Peritoneal Dialysis (CAPD)
- Manual exchanges performed by the patient or caregiver, typically 3–5 times per day
- Each exchange involves draining the used dialysate, infusing fresh solution, and allowing it to dwell for several hours
- No machine is required; treatment is continuous throughout the day
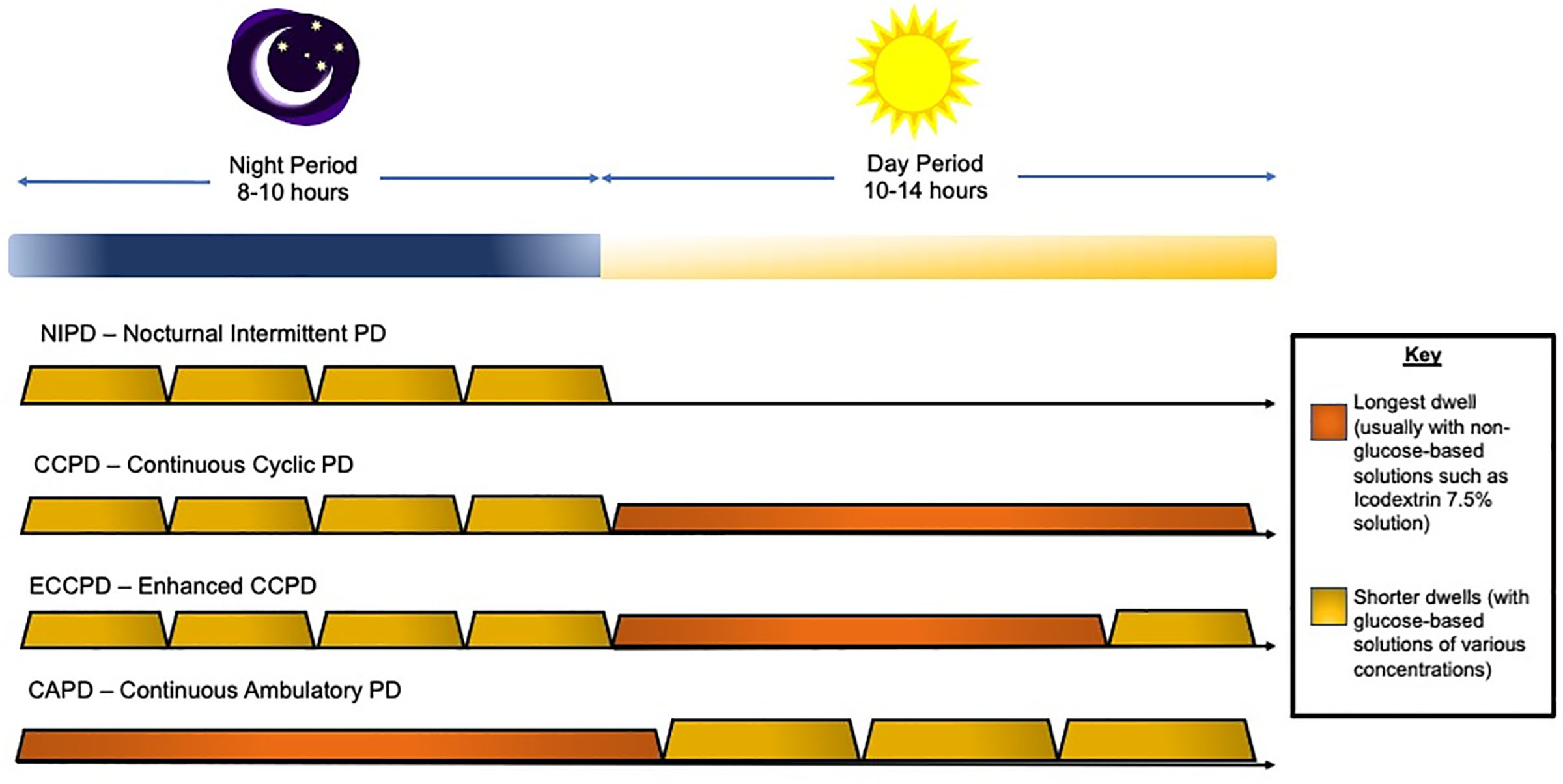
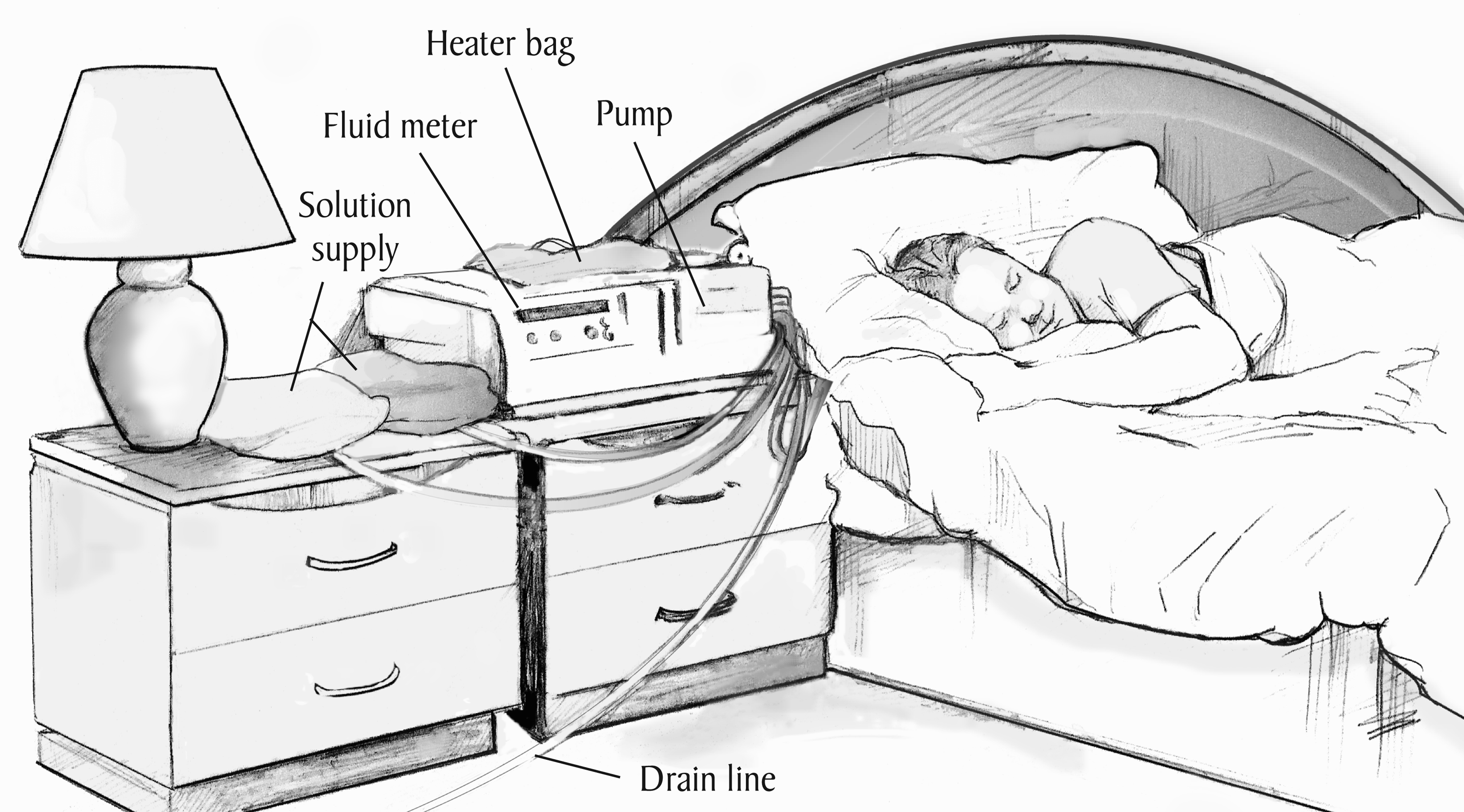
Automated Peritoneal Dialysis (APD) – also called CCPD
- A cycler machine performs multiple exchanges overnight while the patient sleeps
- The patient may wake up "full" (with dialysate dwelling) or "dry" depending on the prescription
- APD can offer more flexibility for school, work, and daytime activities
Indications and Patient Selection
Peritoneal dialysis is one of several options for long-term dialysis in ESKD. It may be chosen for:
- Patients who value home-based, flexible therapy and wish to avoid thrice-weekly in-center HD
- Patients with limited vascular access options or severe vascular disease
- Children and smaller adults where PD can be technically easier and preserve vascular access for the future
- Patients who live far from a dialysis center or have transportation barriers
Selection Considerations
- Ability to perform or supervise sterile exchanges (patient or caregiver), including adequate vision, dexterity, and cognition
- Suitable home environment: clean area for exchanges, storage space for supplies, reliable electricity (especially for APD)
- Medical factors: residual kidney function, abdominal anatomy, hernias, prior major abdominal surgeries, obesity, and comorbidities
Contraindications and Limitations
Absolute or strong contraindications are uncommon but include situations where PD cannot function or would be unsafe.
Examples (often relative and case-dependent)
- Extensive intra-abdominal adhesions or scarring severely limiting dialysate distribution
- Active abdominal wall or intra-abdominal infection (e.g., peritonitis, diverticulitis) until resolved
- Large non-reducible abdominal hernias or severe diaphragmatic defects not corrected surgically
- Severe protein loss or malnutrition that would be worsened by PD
- Inability to safely perform sterile technique at home with no available support
Limitations Compared with Hemodialysis
- Clearance may be less efficient in very large patients or those with high catabolic rates
- Glucose-based solutions can contribute to weight gain, hyperglycemia, and dyslipidemia
- Risk of peritonitis, exit-site, and tunnel infections
- Long-term risk of peritoneal membrane changes (e.g., fibrosis, encapsulating peritoneal sclerosis) with many years of PD
Peritoneal Dialysis Catheter and Access
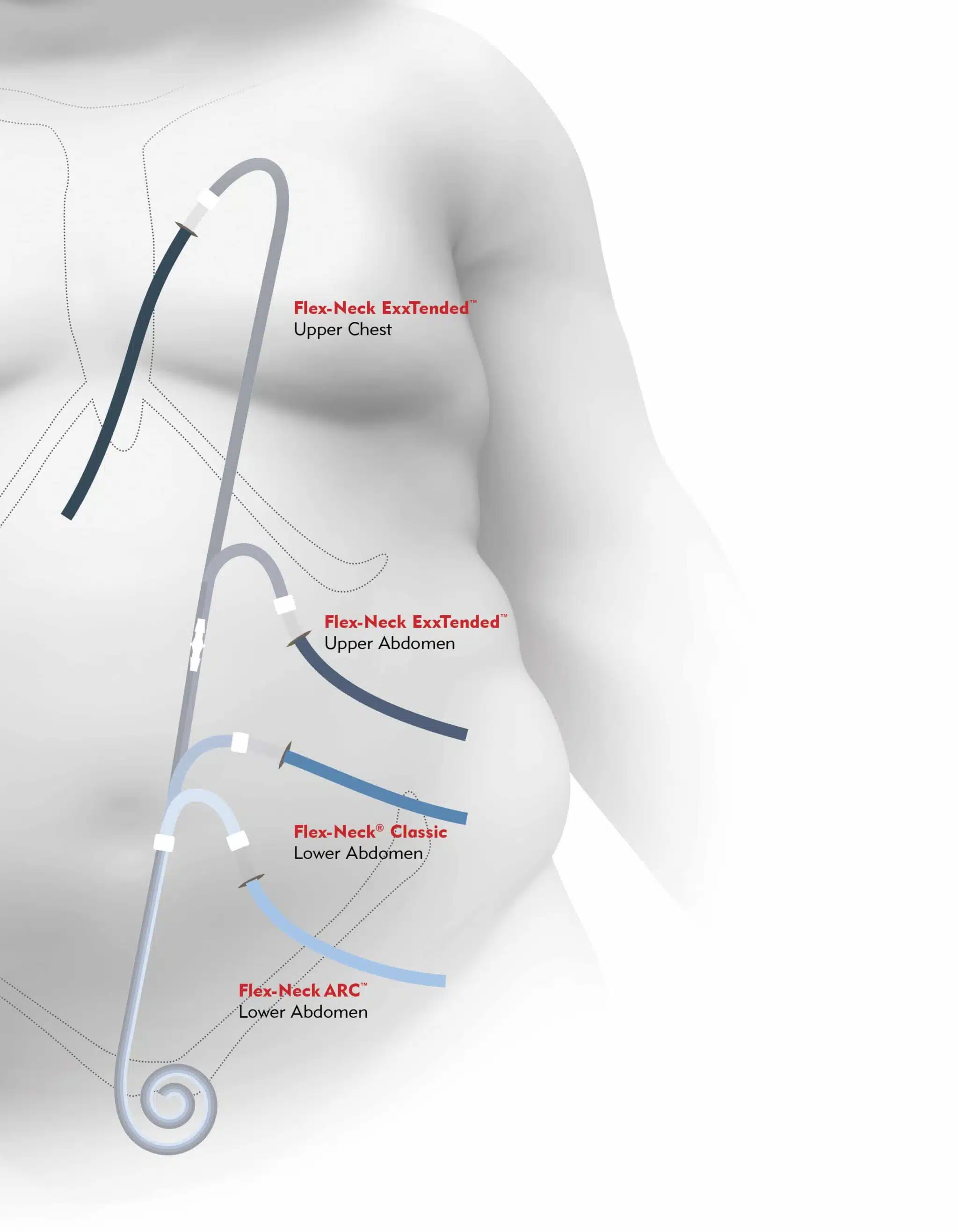
The PD catheter is a soft, flexible tube placed into the peritoneal cavity, usually via laparoscopic or open surgical technique.
Key Features
- The intraperitoneal segment lies in the pelvis, often with curled or coiled tips to reduce migration
- One or two Dacron cuffs sit within the subcutaneous tunnel to anchor the catheter and reduce infection risk
- The exit site is brought out through the abdominal wall where daily cleaning and dressing changes occur
Common Exit Site Locations
- Lower abdomen (below or lateral to the umbilicus), directed downward to reduce contamination and avoid beltlines
- Extended or presternal catheters for patients with obesity, ostomies, or other abdominal issues
Nursing Considerations
- Inspect the exit site every shift (in hospital) and at routine clinic visits for redness, drainage, pain, and crusting
- Teach patients the importance of daily exit-site care and keeping the catheter secure and dry
- Reinforce that the catheter is for PD only—not for infusions, blood draws, or medications
Principles of PD and Basic Prescription
PD works through diffusion and osmosis across the peritoneal membrane:
- Diffusion: Small solutes (urea, creatinine, potassium) move down their concentration gradient from blood to dialysate
- Osmosis/ultrafiltration: Glucose in the dialysate creates an osmotic gradient that pulls water out of the blood into the dialysate
Basic Elements of a PD Prescription
- Type of PD: CAPD vs APD
- Fill volume per exchange: 1.5–3.0 liters per dwell in adults, adjusted for body size and tolerance
- Number of exchanges: Per day (CAPD) or per night (APD)
- Dwell time: How long fluid remains in abdomen (commonly 4–6 hours for daytime CAPD; shorter cycles at night on APD)
Dialysate Strength and Composition
- Glucose concentration (1.5%, 2.5%, 4.25%) to adjust ultrafiltration
- Icodextrin solutions for long dwells to reduce glucose exposure and improve UF
- Calcium and magnesium content tailored to labs and bone-mineral management
CAPD Exchange Workflow (Manual PD)
A typical CAPD exchange (manual PD) involves a structured, aseptic process. Details vary by system (Baxter, Fresenius, etc.), but the core steps are similar:
-
Prepare:
- Perform hand hygiene, wear mask as per local protocol, and set up supplies in a clean, well-lit area
- Check solution bags (clarity, expiration date, correct glucose concentration, and temperature if pre-warmed)
- Inspect catheter and dressing before starting
-
Connect:
- Don mask and perform hand hygiene again
- Connect the PD catheter to the transfer set/system tubing using aseptic technique
-
Drain:
- Open the appropriate clamp to allow used dialysate to drain from abdomen into drain bag
- Observe effluent for clarity, color, fibrin strands, and volume
-
Flush (if applicable):
- Flush a small amount of fresh dialysate to clear the line and reduce contamination risk
-
Fill:
- Infuse the prescribed volume of fresh dialysate into the abdomen
- Clamp lines and disconnect per system protocol
-
Dwell:
- Patient goes about normal activities while dialysate dwells for the prescribed time
-
Disconnect and Secure:
- Ensure catheter is clamped, capped, and secured
- Perform final hand hygiene and dispose of used supplies appropriately
Routine Nursing Monitoring and Care
Key assessments for patients on PD (inpatient or outpatient visits):
Vital Signs and Weight
- Vitals: Blood pressure, heart rate, respiratory rate, SpO₂, temperature
- Weight: Track pre- and post-exchange or daily weight to monitor volume status and UF effectiveness
Intake/Output and Effluent
- Net ultrafiltration (UF): Per exchange or per day; report unusually low or negative UF
- PD effluent: Assess clarity, color, fibrin, and presence of blood or cloudiness
Physical Assessment
- Abdomen: Evaluate for pain, distension, guarding, rebound, and hernias
- Exit site and tunnel: Inspect for redness, drainage, swelling, tenderness, crusting, or overgranulation
Laboratory Monitoring
- Electrolytes, BUN/creatinine, bicarbonate, calcium, phosphate, albumin, and blood counts (per schedule)
Common Complications of Peritoneal Dialysis
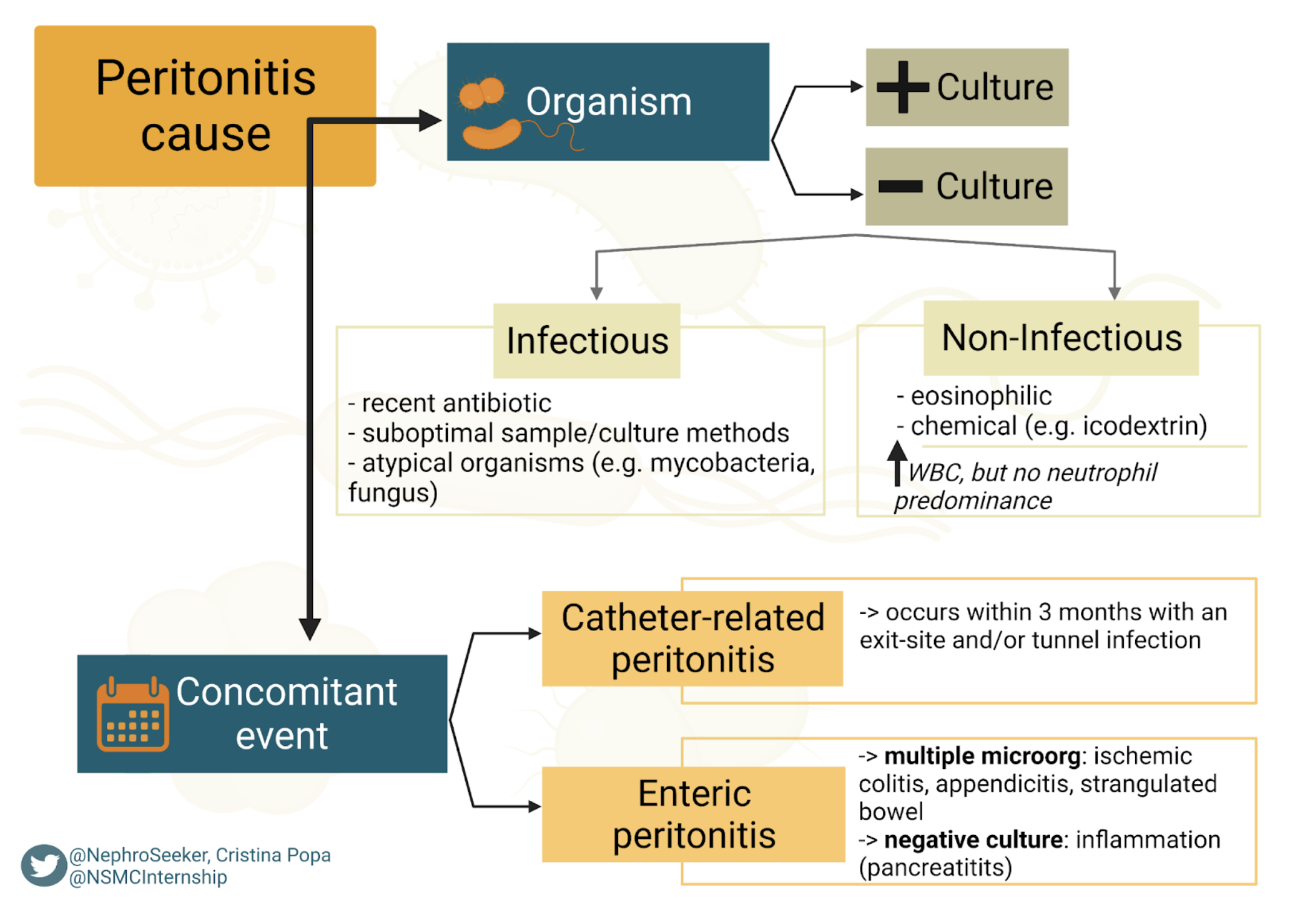
Peritonitis
- The most serious PD-specific complication; usually presents with abdominal pain, cloudy effluent, and sometimes fever or GI symptoms
- Diagnostic criteria: Cloudy effluent with elevated WBC count (e.g., >100 WBC/µL with ≥50% neutrophils) and/or positive culture, per ISPD guidelines
- Management: Intraperitoneal antibiotics directed by local protocols and culture results; may require hospitalization in severe cases
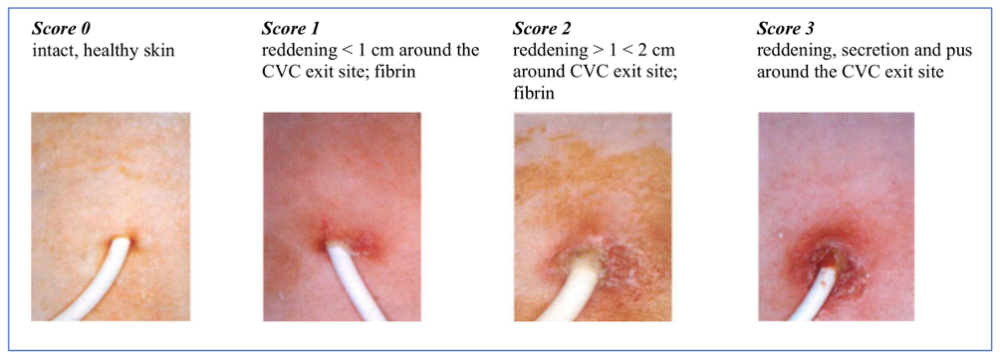
Exit-Site and Tunnel Infections
- Localized erythema, tenderness, or purulent drainage at catheter exit or along tunnel track
- Increase risk of peritonitis; require prompt evaluation and antibiotic therapy per guideline
Mechanical Complications
- Hernias: Umbilical, inguinal, or incisional due to increased intra-abdominal pressure
- Leaks: Around the catheter or into abdominal wall/scrotum
- Catheter malposition: Causing poor drainage or pain
Metabolic Complications
- Hyperglycemia: Due to glucose absorption from dialysate
- Weight gain and dyslipidemia: From chronic glucose load
- Protein loss: In dialysate contributing to hypoalbuminemia and malnutrition
Other Complications
- Back pain or discomfort from dwell volumes
- Encapsulating peritoneal sclerosis (EPS): Rare, severe long-term complication after many years of PD
Infection Prevention and Exit-Site Care
Nursing and patient practices that reduce infection risk:
Aseptic Technique
- Strict hand hygiene and mask use (per local protocol) during connections and disconnections
- Using aseptic technique and closed systems during exchanges
Daily Exit-Site Care
- Cleanse with recommended solution (e.g., antibacterial soap or chlorhexidine) as per program protocol
- Apply topical antibiotic ointment if ordered (e.g., mupirocin or gentamicin) to reduce exit-site infection and peritonitis risk
- Keep the site dry; avoid soaking baths or pools unless specifically cleared
Additional Prevention Measures
- Securing the catheter to prevent traction or trauma to the exit site
- Education on promptly reporting any signs of infection: redness, increased pain, drainage, fever, or cloudy effluent
Patient Education and Self-Management
Core teaching points for patients starting or maintaining PD:
Understanding PD Basics
- How PD works, types of PD, and the purpose of each exchange
- Aseptic technique: hand hygiene, mask use (if indicated), maintaining a clean workspace, and avoiding contaminants (pets, fans, drafts)
Recognizing Complications Early
- Cloudy effluent or new abdominal pain → possible peritonitis; call PD nurse/clinic immediately
- Red, painful, or draining exit site → possible exit-site infection
- Shortness of breath, swelling, or rapid weight gain → possible fluid overload
Medication and Diet Management
- Phosphorus binders, antihypertensives, diabetes control, and any antibiotics or topical treatments related to PD
- Individualized renal diet, fluid limits, and strategies to avoid excessive salt and water intake
Supply and Emergency Management
- Ordering, storing, and rotating PD supplies
- Emergency plans for power outages (for APD) or disasters
- Clear written action plan with phone numbers and timelines for when to seek urgent care vs call clinic
References
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). (2024). Peritoneal dialysis. Retrieved from https://www.niddk.nih.gov/health-information/kidney-disease/kidney-failure/peritoneal-dialysis
- National Kidney Foundation. (n.d.). Peritoneal dialysis. Retrieved from https://www.kidney.org/kidney-topics/peritoneal-dialysis
- Li, P. K.-T., Chow, K. M., Cho, Y., et al. (2022). ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment. Peritoneal Dialysis International, 42(2), 110–153.
- Home Dialysis Central. (n.d.). Peritoneal dialysis (PD). Retrieved from https://homedialysis.org/home-dialysis-basics/peritoneal-dialysis
- Nursing CE Central. (n.d.). Overview of peritoneal dialysis. Retrieved from https://nursingcecentral.com/lessons/overview-of-peritoneal-dialysis/
- International Society for Peritoneal Dialysis (ISPD). (2023). ISPD catheter-related infection recommendations and peritonitis guidelines. Retrieved from https://ispd.org/guidelines/
Medical Disclaimer
- For Educational Purposes Only: This content is intended for educational reference and should not be used for clinical decision-making.
- Not a Substitute for Professional Judgment: Always consult your local protocols, institutional guidelines, and supervising physicians.
- Verify Before Acting: Users are responsible for verifying information through authoritative sources before any clinical application.